- Review

Beyond Surgical Access: Evidence Supporting a Multidimensional Concept of Surgical Invasiveness in Contemporary Cardiac Surgery
- Salvatore Poddi and
- Alessio Rungatscher
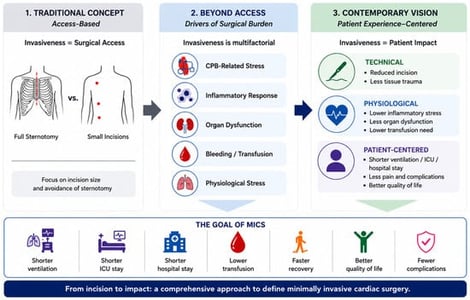
Minimally Invasive Cardiac Surgery (MICS) has traditionally been defined according to the extent of surgical access, primarily focusing on the avoidance of full sternotomy and the reduction in incision size. However, the rapid evolution of cardiac surgery, including technological innovation, robotic platforms, hybrid procedures, and enhanced perioperative management, has progressively challenged the adequacy of purely anatomical definitions of invasiveness. Contemporary surgical practice suggests that the overall impact of a procedure on the patient extends beyond the surgical incision itself and includes several physiological and patient-centered dimensions. This narrative review discusses the contemporary meaning of invasiveness in cardiac surgery and examines the limitations of conventional definitions of MICS based exclusively on surgical exposure. This narrative review is based on a non-systematic literature search of PubMed, Scopus, and Web of Science, and uses a thematic synthesis approach to explore the multidimensional concept of surgical invasiveness in cardiac surgery. Particular attention is given to the growing role of patient-centered outcomes and perioperative burden in defining procedural invasiveness. Building upon emerging conceptual perspectives in the literature, this review highlights a multidimensional interpretation of MICS, in which technical, physiological, and recovery-related factors collectively contribute to the assessment of surgical invasiveness.
8 July 2026